
Mabel Glossary
Below are the definitions and descriptions for commonly used terms or phrases, such as:
Campaign Performance (% Responded, % PNA Yield)
What are % Responded and % PNA Yield and where are they found?
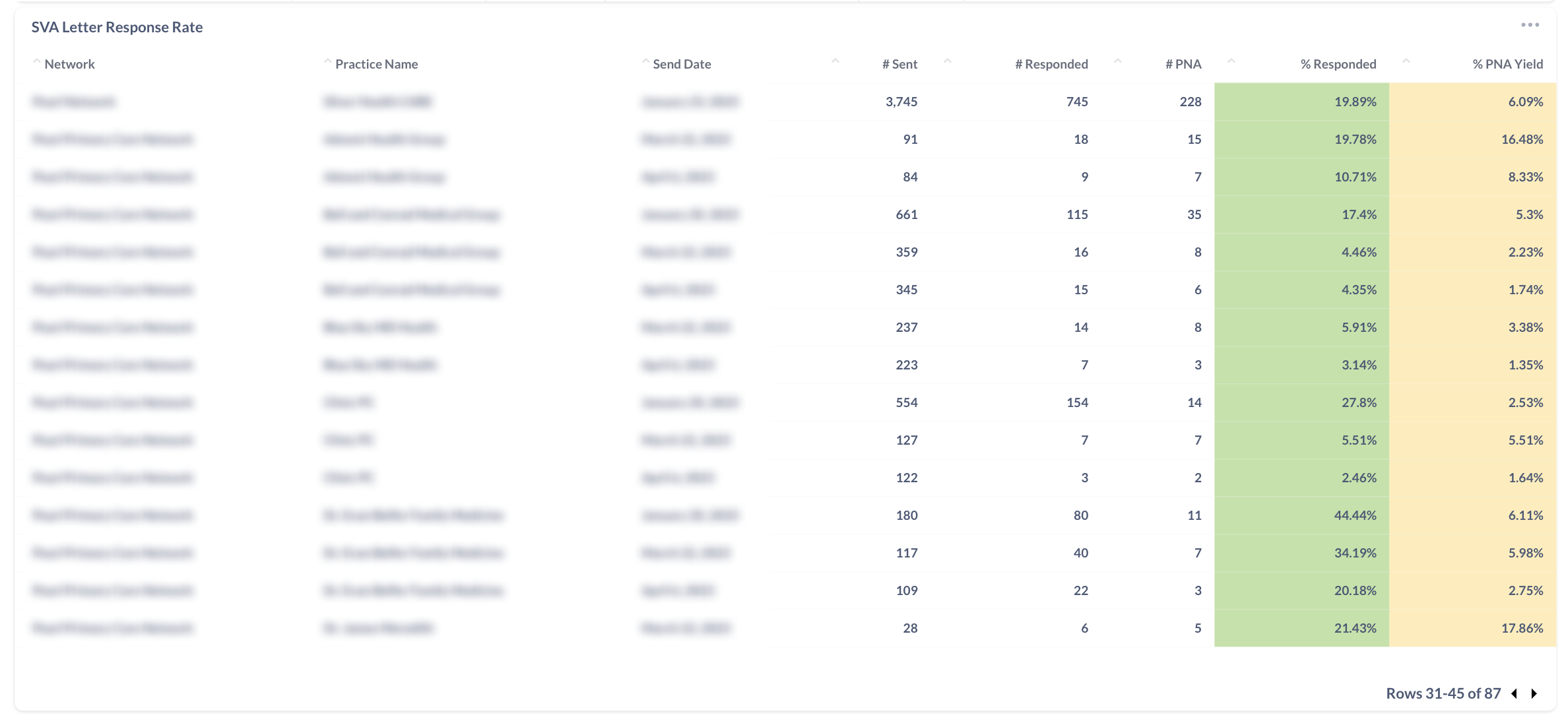
Both are performance measures for any initiative. Specifically, the % Responded is the Total Number of SVA responses / Total Number of Letters or Emails Sent. The % PNA Yield indicates the Total Number of Potential New Alignments / Total letters/emails sent. Since PNA is the key metric that all voluntary alignment initiatives should drive towards, the % PNA Yield is very important to watch. Both values can be found on the Mabel Dashboard, under Campaigns, as the last columns of both the SVA Letter Response Rate and SVA Email Response Rate tables.
Why does the % Responded decrease with every wave?
The % Responded is expected to decrease with every wave (usually by half) as the pool of unaligned beneficiaries who will respond to the campaign begins to saturate.
How does the % PNA Yield inform if we should execute another campaign?
The % PNA Yield directly correlates with ROI for a given campaign. Most ACOs will see a 3x+ ROI for any % PNA Yield >2% and a 5x+ ROI for any % PNA Yield > 4%; Mabel will release a calculator shortly so ACOs can understand this computation and enter in their own values. Nevertheless, any prior campaigns with % PNA Yields of 4%+ should be strongly considered for an additional voluntary alignment campaign.
Why does a particular practice have a low % Responded?
If a low % Responded is experienced on the first wave, there a number of factors to troubleshoot:
Patient List Errors - Incorrect addresses or incorrect subset of patients (i.e. urgent care patient vs. primary care patients) are common causes
Practice name/address errors - incorrect practice names or addresses, or occasionally practices that have recently rebranded, can all result in low % Responded rates for the first wave. Also, campaigns that use an MSO or parent-institution name instead of the individual practice names will similarly lower % Responded rates
Why is there a discrepancy between % Responded and % PNA Yield?
The % PNA Yield can be lower than the % Responded rate for several reasons:
Missing MBIs - when MBIs are missing from a patient list, Mabel is similarly unable to distinguish between existing aligned and unaligned beneficiaries, therefore resulting in a lower % PNA Yield. Re-uploading the patient list with MBIs quickly solves this
Missing Beneficiary Alignment Report (BAR) - if the BAR was unavailable at the time of the mailing, the campaign was unable to distinguish between existing aligned and unaligned beneficiaries, therefore resulting in a lower % PNA Yield
Terminated Participating Providers - if a participating provider/practice is terminated after the campaign has launched, any subsequent SVA responses that cannot be aligned to other NPIs will have to be marked as Invalid, therefore reducing the % PNA Yield
Default Provider NPI
What is the Default Provider NPI? When is it used?
When Mabel receives a completed SVA, we usually submit the NPI associated with the beneficiary in the patient list. However, there are multiple situations where we need to assign a different NPI:
Patient specifies a different NPI - unless the specified NPI is not participating (and thus the SVA is marked as invalid), we update the NPI accordingly
No patient record on file (i.e., new patients, patients who recently switched to Original Medicare, etc.)
NPI on file is invalid (i.e., the NPI on file is for a provider no longer with the practice or with the ACO, etc.)
In the latter two cases, we associate the beneficiary with the Default Provider NPI for the practice. The Default Provider NPI should be the anchor provider or Medical Director of a practice.
How can I access the current list of Default Provider NPIs for my ACO?
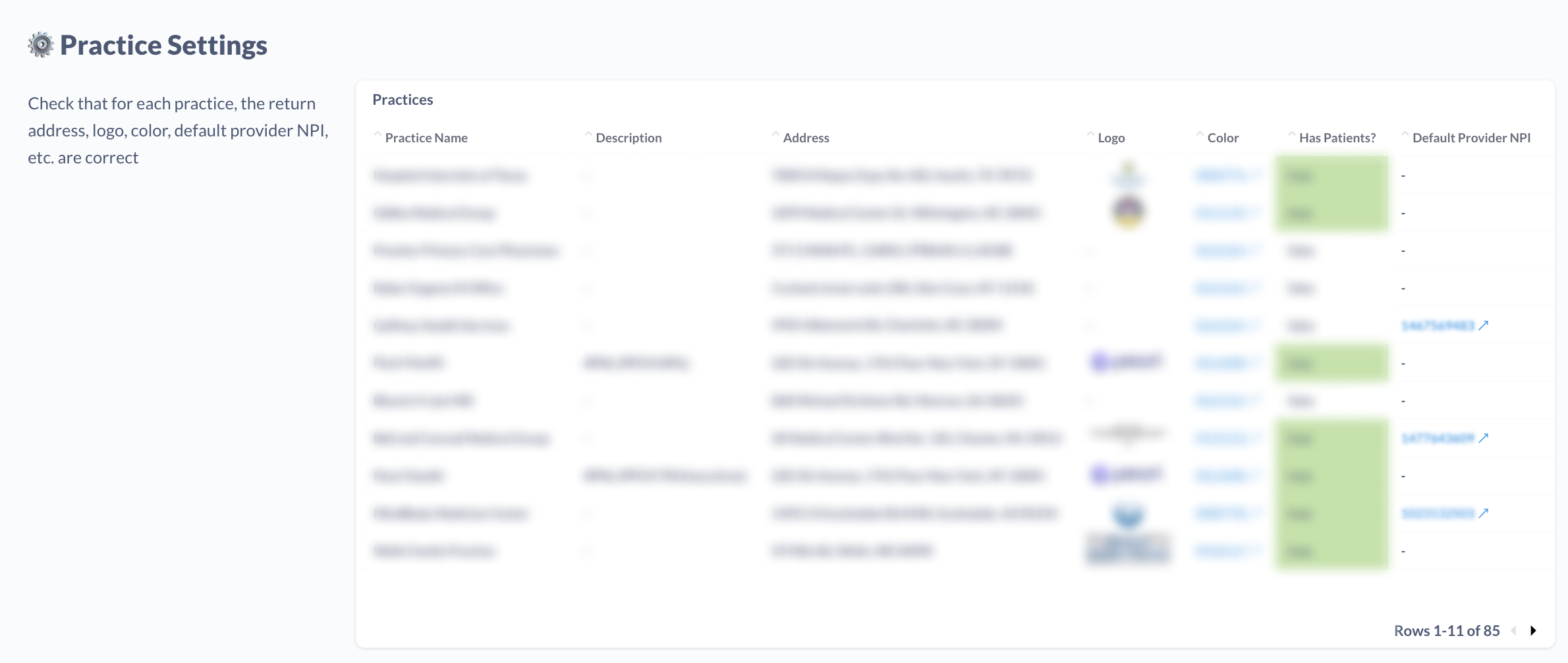
The list of Default Provider NPIs can be found on the Mabel Dashboards, under “Setup”, scroll down to “Practice Settings”. For each practice/row, there is a “Default Provider NPI” column where the NPI is defined. This list can be downloaded by hovering over the top right corner of the table, clicking the ••• and selecting “Download as .xlsx”.
What is the process for changing the Default Provider NPIs assigned in my network?
Upon downloading the the Practice Settings for your ACO, please update the Default Provider NPIs column with your updated NPI and highlight the cell so the Mabel team knows which cells have been updated. Send your updated spreadsheet to support@getmabel.com and our team will incorporate the changes.
Practice Settings
Why are there additional practices in my network?
Mabel creates several additional practices for every ACO network to support various functions:
<ACO Name> - Practices with “#BNL” in the description are used to send out Beneficiary Notification Letters
<ACO Name> - Unaffiliated - this is a virtual practice created to house beneficiaries who do not appear in a network’s patient lists, yet the beneficiary has completed an alignment form. As of June 2023, most of the Mabel Dashboard analytics abstract this practice away and attribute patients to their respective practices
There is a practice listed that is no longer participating in our ACO REACH. Can it be removed?
Before reaching out to support@getmabel.com, please confirm that the Practice has not already been archived. Archived practices will have the row highlighted in RED; also, under the “Archived?” column, the value will be “true”. Archived practices are no longer participating in campaigns. However, any completed alignments tied to patients within archived practices will still be submitted to CMS.
What makes a good practice logo?
The print space for practice logos is usually 2.4in width x 1in height, so the ideal logo is one that is a) wide vs. tall, since a tall logo will be scaled down to fit in the space, and b) big enough (in size or higher resolution) so it will print cleanly in that space.
Potential New Alignments (PNA)
How is PNA calculated?
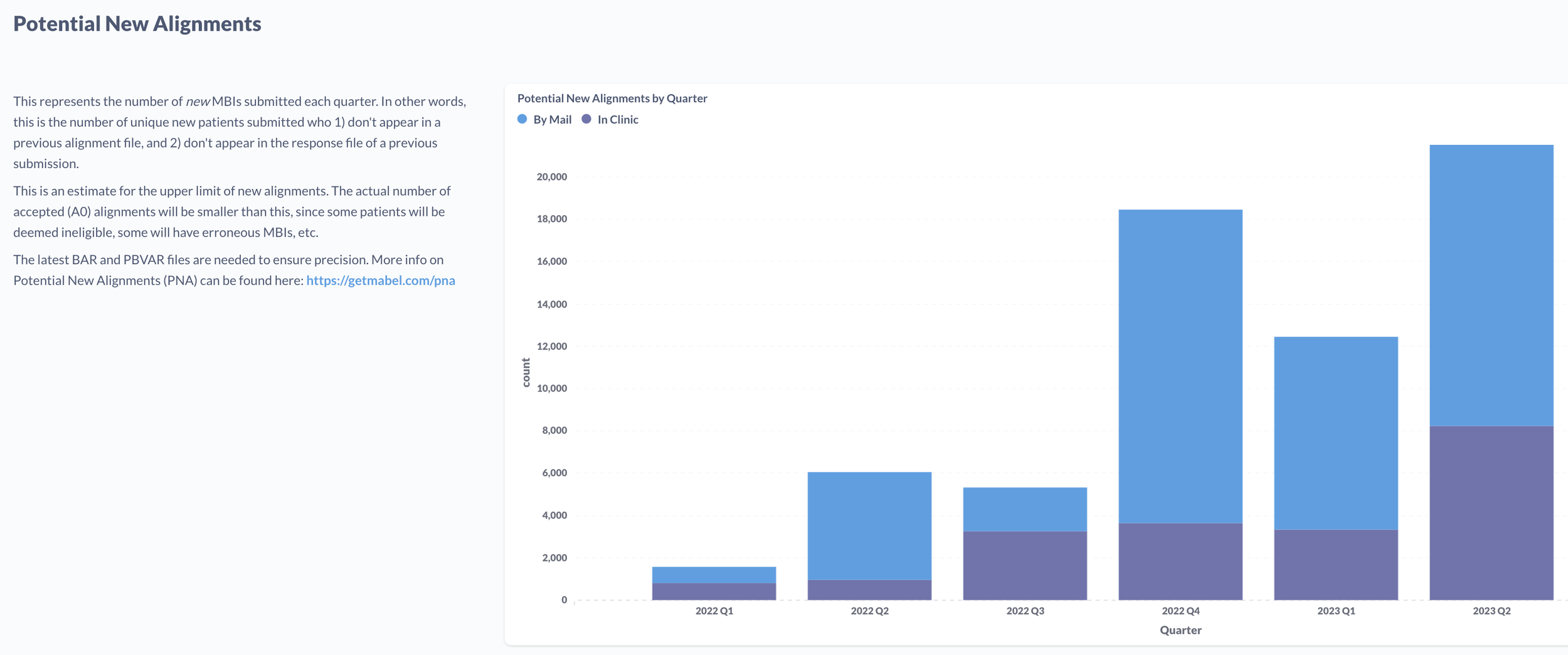
The Potential New Alignments are computed by taking the CMS Submission file (unique MBIs only) and excluding already-aligned beneficiaries as well as any previously submitted alignments.
Why is PNA important?
It is the most relevant metric to share with leadership to inform forecasting/projections. The Actual New Alignments (A0, as reported by CMS) varies by network, but tends to come in at ~65% * PNA for Standard ACOs and ~40% * PNA for High Needs ACOs.
Why is there a difference between the number of Completed SVAs and the number of rows in the submission file?
Per CMS guidance, Mabel only submits the most recent Completed SVA per MBI. If a patient signs multiple SVAs (e.g. both by mail and also in their provider’s office), the SVA with the most recent date will be included in the CMS submission file. Moreover, Mabel filters the submission list for SVAs that have not appeared in a previous SVA response file, again per CMS guidance.